Background Reading
Effect of functional electrical stimulation (FES) assisted rowing on cardiorespiratory function in persons with spinal cord injury
People with spinal cord injury (SCI) are at an increased risk of the diseases of inactivity (cardiovascular disease, diabetes, osteoporosis and obesity) compared with their able bodied counterparts. In addition, some of the physiological consequences of SCI (e.g. impaired bladder, bowel and sexual function) result in a reduced quality of life. Improvements in cardiorespiratory fitness are related to a reduced incidence of the diseases of inactivity and an enhanced quality of life in people with SCI. To improve cardiorespiratory fitness an appropriate exercise training programme is required. Such a programme needs to place the cardiorespiratory system under sufficient stress to stimulate adaptation. Neither upper body exercise nor functional electrical stimulation (FES)-assisted cycling appear to provide sufficient physiologic stress to bring about significant improvements in cardiorespiratory fitness.
Hybrid functional electrical stimulation (FES)-assisted exercise systems, which recruit the paralysed lower limbs simultaneous with the voluntary action of the arms, significantly increase the cardiorespiratory demand of exercise. FES-rowing has been shown to elicit a greater acute cardiorespiratory response than any other type of exercise in people with SCI. It is possible, therefore, that people with SCI may derive significant cardiorespiratory benefits from a programme of FES-rowing training.
Studies that have investigated the cardiorespiratory benefits of FES rowing have focused on gross measures of aerobic capacity. Although important, these studies have not examined the effect of FES-rowing upon the physiological systems that underpin changes in cardiorespiratory fitness. Cardiac, vascular and respiratory structure and function may all change in response to a structured programme of FES-rowing. Therefore, the purpose of the present study is to determine how the physiologic systems underpinning cardiorespiratory fitness and quality of life adapt in response to a programme of FES-rowing. Such information may ultimately provide a basis for using FES-rowing training as an additional therapeutic measure in people with SCI.
--------------------------------------------------------------------------------
The Potential Therapeutic Benefit of Cortical Repetitive Transcranial Magnetic Stimulation on Pelvic Sphincter “Guarding Reflex” Function To Promote Continence In Incomplete Spinal Cord Injury: A Pilot Study
Bladder and bowel problems continue to be the most troublesome aspects of everyday life for people with paraplegia. Indeed, recent surveys have shown that above all the many other medical conditions in spinal cord injury, the need to continue targeting recovery of bladder, bowel and sexual functions are uppermost in patients’ own desires; this is despite the considerable progress achieved to manage them over the past 60 years. There are a number of treatments to alleviate the bothersome symptoms of urinary and faecal incontinence including drugs, medical devices and surgery, but none are completely satisfactory. Furthermore, the so-called “cure” by nerve regeneration and repair, if it is possible, is now looking likely to require many more years of development . So it is timely to consider some alternative therapies that might be achievable in the shorter-term. One such new therapy could involve tapping into the “plasticity” of surviving nervous pathways in the spinal cord following an injury; pathways that normally control voluntary contractions of the bladder and bowel sphincters that help to maintain continence and achieve voiding.
Recently, our team, at the London Spinal Cord Injuries Centre at Stanmore, together with Imperial College and University College London, has been investigating the integrity and function of any elements of the spinal pathways controlling bladder and bowel sphincters that have survived in people with incomplete spinal cord injuries. When compared to people without an injury we have found, not unexpectedly, that voluntary sphincter contractions are weak, variable and poorly sustained. Interestingly, when we stimulate these residual spinal pathways with a single non-invasive magnetic stimulation pulse to the correct part of the brain we can momentarily enhance reflexes that contract the sphincters, but only to a much lower level as compared with people without a spinal injury. In neither group of people do we observe this enhancing effect lasting longer than a few seconds at most. Clearly such brief interaction does not impact significantly on the plasticity of the brain or spinal cord and provides no lasting functional benefits.
However, studies of limb muscles have shown that by giving bursts of repetitive magnetic transcranial stimulation (known as rTMS) to the brain, the voluntary pathways to muscles can be significantly facilitated and the effects made to persist for up to many hours or even days. We suggest that the potential for extending these persistent effects to bladder and bowel sphincters may well be the basis of a therapy, for example as an adjunct to proven rehabilitation techniques, to improve continence in spinal cord injury. In a small preliminary study on healthy volunteers we have already demonstrated the utility of rTMS for enhancing sphincter reflex function. This application is now for funding a pilot study to investigate, in a randomized scientifically controlled way, whether similar effects can be demonstrated in persons with an incomplete spinal cord injury. If we are successful in this endeavour then we would go on to develop a more comprehensive study to investigate the impact of such important effects on improving continence and voiding in spinal cord injury.
--------------------------------------------------------------------------------
What are the views of people with Spinal Cord Injury (SCI), healthcare professionals and researchers about the current and future use of FES?
For nearly half a century Functional Electrical Stimulation (FES) has been used in the treatment and management of physical problems encountered by people with SCI. Applications have encompassed bladder and bowel control, pain, movement, tissue viability and musculoskeletal and cardio-respiratory function. Although there appears to be a growing body of research developing and evaluating these techniques, it is generally found they have only been used by a small fraction of the SCI community.
While techniques have evolved to be more effective and technically sophisticated, they have often undergone phases of great popularity followed by periods of rejection. Popularity has often been associated with highly active research groups and faded with loss of funding of research or a failure to achieve technology or clinical transfer. In order to address issues related to problems with transferability and application to clinical practice, it is important to ensure that future developments in FES are patient-led and fulfil the needs of people with spinal cord injury. Developments encompass research, technology development, clinical and service provision and commercialisation. Unless each of these is driven by the needs of the SCI community then the money and time invested may be wasted. It could be argued, that to continue without this knowledge is an unethical use of public funds and the time and energy of people with SCI.
Although the first stage of the programme of research has provided an important insight into some of the key issues regarding the current and future use of FES, this qualitative approach involved in-depth methods that gather the views of a relatively small group of people. Therefore, the second stage of this research is to use the themes identified in the qualitative study to develop a series of questionnaires that will explore the extent to which the wider SCI community hold these views. This will involve carrying out an international study with a much large sample of people.
--------------------------------------------------------------------------------
Central Nervous System (CNS) reorganisation after spinal cord injury: its relationship to pain and response to mental imagery.
Below level pain (phantom pain) in the Spinal Cord Injured (SCI) is common, often severe and difficult to treat with conventional medicines. The causes of this pain are complex, with experiments showing changes in electrical activity in all areas of the brain, related to the loss of normal sensation and movement. The relationship between below level pain and changes in brain activity has not been established in humans with spinal cord injury. The development of specialised brain scans known as functional Magnetic Resonance Imaging (fMRI) allows us to investigate this relationship in a non-invasive, non-radiation manner. Using fMRI, it has been shown in previous research that people with phantom pain can be helped by teaching them to “move” and “feel” their phantom limb, and that this pain reduction is linked to a normalisation of brain activity. In a more recent pilot study (funded by INSPIRE) it was found that changes in brain activity were more extensive in people with spinal cord injury (SCI) and below level pain compared to those with SCI and no pain and healthy controls. It was also found that, when participants with below level pain were taught to practice regular imagined movement and sensation in the paralysed, painful areas, it was possible for this imagination to relieve the pain and reduce the abnormal patterns of activity. In effect, using the brain’s own powers to heal itself. The pilot study has helped to refine the technique, show that fMRI can measure brain changes in the spinally injured and take note of the comments of those who participated.
This application intends to expand on these promising results by studying a larger group of participants (a total of 20 in each of the 3 groups [SCI with pain, SCI without pain and healthy controls] including those from the pilot). All participants will be scanned at the outset of the study, and brain activation in response to tasks such as blowing a kiss, moving the fingers, imagining movement of the toes will be measured. The two SCI groups will then undergo the therapy, which will consist of 6 x one hour sessions with the therapist plus a CD for home practice. The group with pain will learn a simple relaxation technique plus imagining normal movement and sensation in the paralysed or painful limbs. At the end of therapy the SCI participants will be re-scanned. A careful record will be kept of pain scores throughout the study. At six months all participants will be interviewed and asked to keep a final diary so the long term effect of the intervention can be measured.
It is hoped that this study will benefit the wider SCI community in two ways. First, if the clinical therapy is successful, a CD of the therapy would be available for general distribution, plus training for health care professionals involved in the care of people with SCI. Secondly, the information from the brain scans will help researchers and clinicians to learn more about the effect of SCI on the function of the brain, and the mechanisms behind this most distressing pain condition. Moreover, the brain imaging results, showing the extent of activation in the motor cortex of the brain may be useful to those seeking to improve mobility after spinal injury.
--------------------------------------------------------------------------------
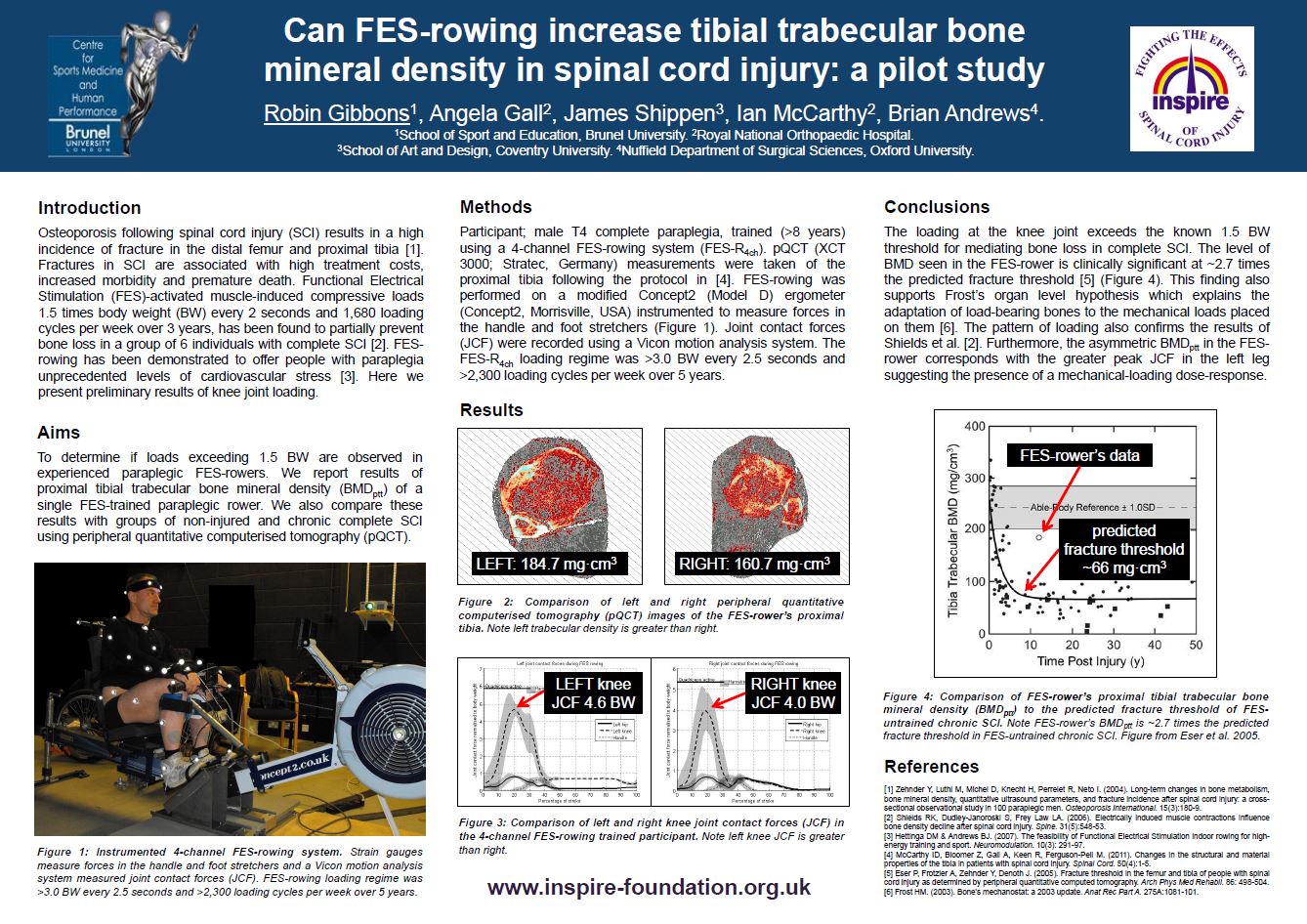
An INSPIRE funded pilot study conducted at Brunel University demonstrating the effects of FES-Rowing on bone density in the legs after spinal cord injury.